Jose L. Agraz, PhD
Finger Force
Finger Force : Anatomy
Anatomy of the Hand
The purpose of this thesis is to describe a force-measuring device that
records single- and multiple-finger force profiles. The force profile that is produced is
a function of the anatomical and physiological systems that control the digits. Thus a
brief overview of the anatomy and physiology of the hand is necessary to better
understand the finger force-profiles.
The bones of the hand consist of three segments: the wrist bones called the
carpus, the bone in the palm called the metacarpus, and the individual bones of the
fingers are called the phalanges.
The U.S. Department of Labor (DoL) concluded that the CTS is the “Chief
occupational hazard of the 90’s”, affecting around eight million Americans and
accounting for 41% of all work-related injuries. It is estimated that 25% of all
computer operators have CTS, and by the year 2000 the DoL estimates over 50% of
the workforce may be affected. Approximately 20,000 medical procedures are
performed every year to correct various aspects of CTS; however, only 23% of all
CTS patients are able to return to their previous professions after surgery.
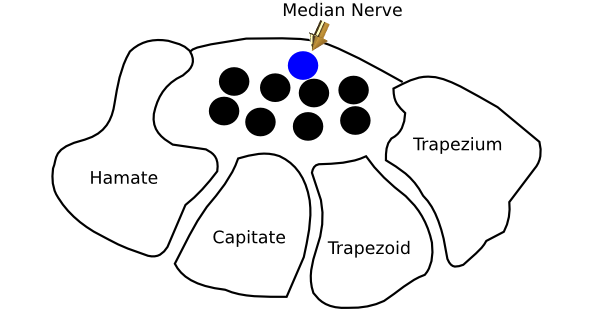
The eight wrist (carpal) bones are arranged in two rows. The lower row starts
from the thumb to the little finger (radial to lunar side), and the second row leads to
the metacarpals. Although there are extensive articulations between the various wrist
bones, the attachments of muscles to them do not significantly impact on finger
performance.
The carpus overall is concave anteriorly and a ligament overlays this
concavity forming the infamous carpal tunnel. This tunnel contains the median nerve
and several long muscle tendons. Overuse and inflammation of the tendons
compress the median nerve, which then influences the muscles that this nerve
innervates, which influences finger movement and force development.
The five metacarpal bones of the palm have a number of important members.
The metacarpal bone of the thumb is shorter and wider than the other metacarpals
and is anatomically configured to accomplish the complex motor movements of the
thumb. The base has a concavo-convex surface for articulation with the carpal bone,
the trapezium, allowing for a wide range of movement. The thumb metacarpal has
four different sets of muscles attached to it. The metacarpal bone of the index finger
is the longest followed by middle, ring and little finger metacarpals. Each of these
bones has multiple muscle attachments.
The phalanges are the bones of the fingers, of which there is a total of
fourteen, three for each finger and two for the thumb. They are considered long
bones and their distal ends are smaller than their proximal ends, which allows for
each succeeding finger to articulate smoothly with the proceeding finger.
The first row of phalanges articulate with the metacarpals and the second row
of phalanges; the second row of phalanges articulate with the first and third row of
phalanges and the third and final row articulate with the second row
Muscles that Move the Wrist and Fingers
The muscles that move the bones of the hand are either in the forearm, the extrinsic muscles, or are in the hand itself, the intrinsic muscles. The extrinsic groups of forearm muscles are both superficial and deep. The anterior superficial and deep muscles collectively flex the wrist and/or fingers. The posterior muscles of the forearm are divided into four categories; superficial, deep, intrinsic and extensor. The superficial and deep muscles, control extension of the wrist and fingers and also the fanning of the fingers. The intrinsic muscles are located in the hand per se and are best demonstrated by the lumbricals that cause the phalanges to fan when the hand is spread wide.
Innervation of the Forearm and Wrist
Innervation of the muscles of the forearm and the hand are derived from the median, ulnar and radial nerves that originate from the cervical (neck) regions C5-C8 and thoracic (upper back) T1 vertebrae. The median nerve controls the flexor groups of the forearm as well as the intrinsic muscle of the lateral palm and first two fingers. The ulnar nerve controls the flexor muscles in the anterior forearm and most of the intrinsic muscles of hand. The radial nerve innervates primarily the extensor muscles of the forearm and wrist.
Muscle Contraction
There are two types of muscle contraction that the fingers perform: isometric and isotonic. Isometric contraction involves the contraction of the muscle without a change in the length of that muscle. Isometric contraction occurs when the person continuously depresses the key and not releases it. Isotonic contraction refers to a change in the length of the muscle while a constant force is being generated. Isotonic contraction is best exemplified when the fingers depresses and releases a key.
Physiology of Finger Movement
The large portion of the motor and sensory cortex that’s devoted towards
finger movement manifests the importance of control of finger movement. Studies of
the mechanism(s) of coordinated sequential finger movements and force generation
have been few. The scientific literature is rich with studies dealing with force
generation of the limbs but hardly any exists that deals with fingers. The seemingly
simplistic act of striking a key involves a number of steps that begins when the motor
command is generated in the motor cortex, travels to specific areas of the spinal cord
and then activates various wrist stabilizers and finger flexors and extensors.
Under normal circumstances, the finger force generated is sensed by various
biomechanical sensors located in the muscles and joints of the fingers and wrist and
is transmitted back to the spinal cord and higher centers. Hagbarth et. al. reported
that the receptor for stretch in the finger muscles and the muscle spindle, play a role
in controlling the stiffness of the forearm and finger muscles. Birznieks et al
reported that local friction on the surface of an object influences the amount of force
produced by the fingers, suggesting that skin sensors also influence the amount of
force generated.
Finger-Force Production
Finger force is generated when the muscles of the forearm and intrinsic
muscle of the hand contract to depress a key. Parlitz, Peschel and Altenmuller, used
resistive sensors to measure the dynamic finger force produced by musicians and
non-musicians as they performed three different exercises of increasing difficulty.
They used a commercially available force-scan matrix fold (sensor array layers)
(Tekscan), which contained 960 sensors per foil. The sensors were placed beneath
five adjacent white keys on a grand piano. Their data suggested that mean force per
touch and the mean touch duration for each exercise was greater in the non-trained
subjects than in those trained. Martin et. al. studied the relationship between the
surface electromyogram of the forearm muscles and the keyboard reaction forces in
ten persons who executed a keyboard task performed at a comfortable speed.
Reaction forces were measured using a pair of load cells (conditioned force sensor)
placed under the computer keyboard. Subjects were asked to type paragraphs that
had all the letters of the alphabet. Peak forces ranged from 1.84 to 3.3N with an
overall average of 2.59N, which is 5.4 times the Key Depression Force (the minimum
force necessary to close the key switch). The force profile was greatest for the
thumb, followed by the middle finger, then the index, ring and little fingers. Women
generated twice as much force as men. Since the interkey delay ranged from 109 to
256 milliseconds (ms) and the keystroke duration was only 100-120ms, the authors
concluded that the strokes were not influenced by feedback loops from the muscles
or joints.
Gerard et. al. studied the effect of key stiffness on the development of fatigue,
keyboard reaction forces and muscle electromyography. A strain gauge mounted
under the keyboard amplified the force generated at the keys. They reported that
subjects who typed for two hours generated four times the minimum force needed to
depress a key and that the ratio of typing force to the electromyogram of the flexor
muscles was not a good indicator of fatigue
In a report presented on the World Wide Web, Dennerlein, Mote and Rempel
studied the question of whether or not the index finger motion, forces and
electromyogram were ballistic. Although they studied only one subject they
presented data correlating the finger position, force and electromyogram. Force was
measured with a load cell placed underneath the J key on a standard computer
keyboard. Based on the bursting pattern of the EMG, associated with the activation
of the forearm extensor muscle, followed by the activation of the forearm flexor
muscle and subsequently the extensor muscle, they concluded that the finger
depression on the key is ballistic. Meinck et al reported a three-burst pattern of
the extensor and flexor electromyogram during finger flexion. They also concluded
that finger flexion on the keyboard was a ballistic movement.
In addition to the force profiles produced during finger flexion, there is an
associated high-frequency tremor of 8-12 Hz found in the electromyogram. This
frequency is associated with the synchronization of the motor units firing at that rate
 Introduction
Introduction
 Anatomy
Anatomy
 Methods
Methods
 Results
Results
Feb 14th, 2015 at 5:09 pm