Jose L. Agraz, PhD
Finger Force
Finger Force : Introduction
Statement of the Problem
Repetitive Stress Injury (RSI) is attributed to a number of overlying
biomedical factors. Repetitive activities performed at work or leisure over an
extended period of time, constant excessive load or effort and poor body mechanics
are suggested as causes of RSI. In addition, medical conditions such as pregnancy,
rheumatoid arthritis, and diabetes can also contribute to RSI. When RSI occurs at
the wrist and/or fingers, persons complain of numbness, tingling and pain in the area
of the thumb, index, and middle fingers. The pain often increases at night and can
radiate to the forearm, upper arm and neck. Eventually the affected person loses
strength in the affected hand and can no longer easily move the fingers.
The term given for this set of symptoms is carpal tunnel syndrome (CTS),
which is the narrowing of the anatomical tunnel formed by the wrist (carpal) bones
through which the median nerve travels. The compression of the median
nerve influences its sensory and motor innervations to the thumb, index, and middle
fingers causing tingling, numbness, burning sensation, weakness and clumsiness.
The U.S. Department of Labor (DoL) concluded that the CTS is the “Chief
occupational hazard of the 90’s”, affecting around eight million Americans and
accounting for 41% of all work-related injuries. It is estimated that 25% of all
computer operators have CTS, and by the year 2000 the DoL estimates over 50% of
the workforce may be affected. Approximately 20,000 medical procedures are
performed every year to correct various aspects of CTS; however, only 23% of all
CTS patients are able to return to their previous professions after surgery.
Women are twice as likely to develop CTS as their male counterparts.
Although they comprise 45% of the work force, they experience 66% of all work-
related repetitive stress injuries.
The Occupational Safety and Health Administration (OSHA) estimates that by
the year 2000, cumulative trauma syndromes will account for 50 cents of each dollar
spent on medical care. The American Academy of Orthopedic Surgeons estimates
that CTS cost 1 billion dollars annually in medial treatment. Each worker
compensation claim for repetitive stress injuries can cost from $20-100K.
Keyboard usage exacerbates other repetitive actions that are associated with
CTS. Carpal Tunnel Syndrome, and its associated pathologies, is common among
persons who use keyboards or fretboards as well as flute and string players.
Treatment options for CTS vary widely, they include; surgery, Yoga, wrist
splints that minimize wrist movements, specialized exercise equipment that
strengthen the muscles of the forearm and fingers, and psychological support after
the injury. The rationale for Yoga is that stretching and relaxing the wrist and forearm
musculature can minimize CTS. Wrist splints can often help, especially within three
months of the onset of symptoms. Their use reduces the latency of the evoked
electromyogram (EMG) of the median nerve. The latency measurement of the
median EMG is considered the criterion standard for the diagnosis of CTS.
Various exercise devices have also been reported to be effective. Flextend is an
example of such a device designed to correct the imbalance between the flexor and
extensor muscles of the wrist. Flexor muscles of the forearm are more powerful than
the extensor muscles and may contribute to the onset and progression of CTS.
The diagnosis of carpal tunnel syndrome is difficult. The classic procedure
used to detect CTS via latency times of the median nerve and/or clinical evaluations
have indicated that these two methods are not adequate to identify all patients who
have the symptoms of CTS. Another method commonly used by the clinician is to
evaluate the grip strength of the patient. This procedure requires the patient to
maintain a constant amount of force for a minute or to rapidly grip and release a
force-measuring device (dynamometer). This procedure does not mimic the real
world, and its value as a diagnostic tool is questionable.
At present there is no objective measurement of the force that the fingers can
produce when they are sequentially generating force on a keyboard while controlling
the wrist angle. Although CTS is a major problem facing the work force and
recreational groups in the United States, there is no reported method that quantifies
pre- and post-finger force values after clinical intervention. In addition, there are no
standards (e.g.: databases) of how much force one or all the fingers can generate
while typing in a controlled situation. To develop such a database, a system is
needed to collect and analyze finger-force data.
Background and Significance
At present the diagnosis of CTS remains controversial. Atcheson, Ward and
Lowe evaluated 297 patients of whom 38% were diagnosed with CTS and studied
whether there were any underlying pathologies that may contribute to the diagnosis
of CTS. They concluded that a person with CTS is one who complains only of pain
in his/her upper limb.
The subjective criteria for diagnosis CTS consisted of the following:
- At least one prior CTS diagnosis by a practitioner
- The National Institutes of Occupational Safety and Health criteria for diagnosis of work-related CTS
- Examiner's global assessment of CTS made by the examining physician, paired with clinical CTS criteria, and a distribution of the median nerve spreading of neuropathic symptoms.
OSHA has proposed that slowing of conduction velocity in the median nerve in the carpal tunnel may be related to such non-workplace variables as age, obesity, wrist dimensions and physical inactivity. However, physical inactivity can slow conduction velocity even more than repetitive forceful hand or finger use. Persons with CTS may also have problems associated with the tendons that connect the muscles to the fingers. Patients may complain of tendinitis, inflammation of a tendon the resulting in pain, tenderness and swelling and/or tenosynovitis, which is inflammation of a tendon sheath that covers and protects tendons at joints, causing pain, swelling, tenderness and functional disability.
Statement of Purpose
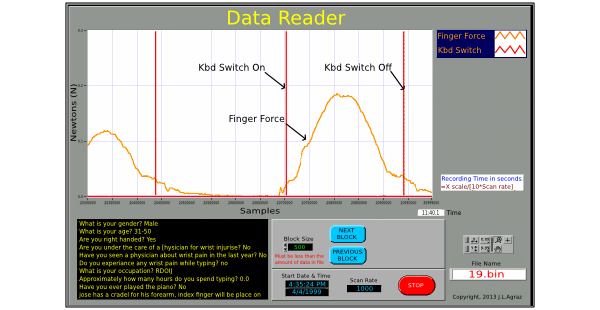
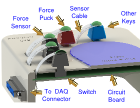
The purpose of this project is to describe a force-measuring device that records single- and multiple-fingers force profiles. This system will incorporate individual force sensors on an ergonomically designed and commercially available computer keyboard. In addition, software will be developed to record the subject's depression and release of single and multiple keys and the force profile of each finger-force level.
 Introduction
Introduction
 Anatomy
Anatomy
 Methods
Methods
 Results
Results
Feb 14th, 2015 at 5:09 pm